About
Investing in women, children and adolescents is one of the most impactful actions a country can make. It improves population health, empowers women to be agents of change in their communities, and puts countries on a path towards development and prosperity.
The Global Financing Facility (GFF) is a country-led partnership, hosted at the World Bank, that fights poverty and inequity by advancing the health and rights of women, children and adolescents. It does this by supporting countries to strengthen health systems and improve access to care through prioritized plans, aligned public and private financing, and policy reform.

More countries are prioritizing and scaling up investments to strengthen primary care and service delivery and are promoting sustainable, equitable financing so that all women, children and adolescents can access quality care.

71% of GFF partner countries implementing their investment case for five or more years report improvements across essential care, including assisted deliveries, pregnancy and newborn care, childhood immunization, and family planning.
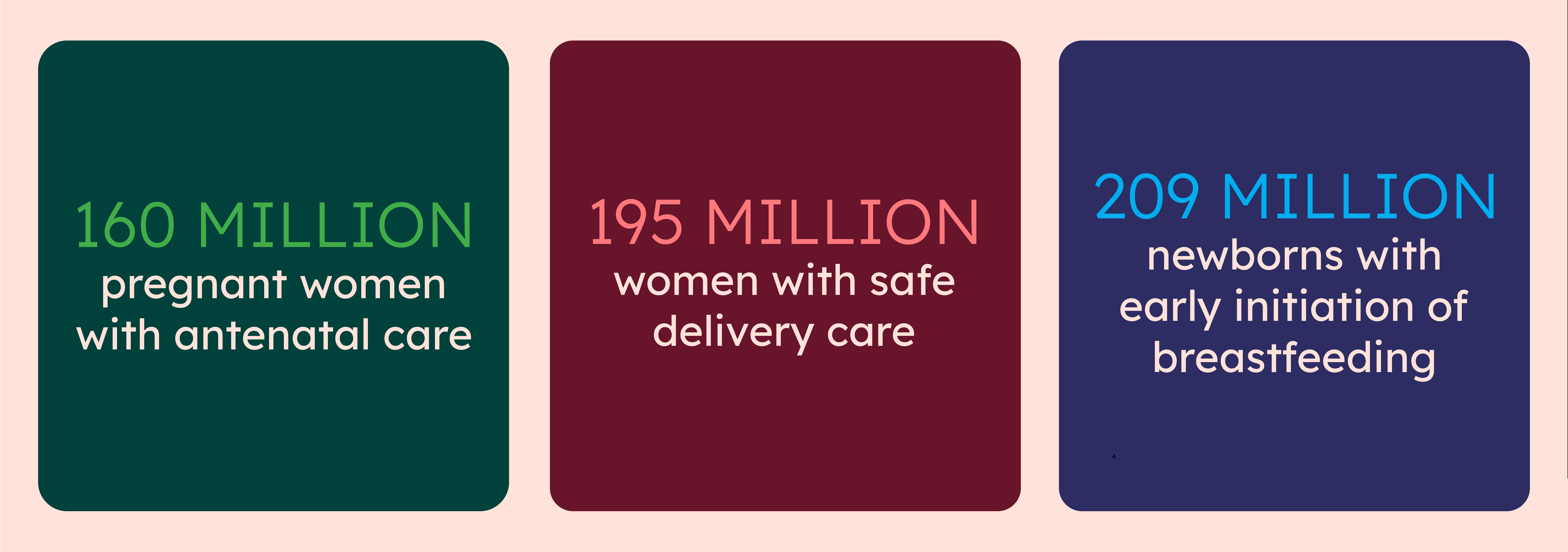
To date, the partnership has helped countries reach millions of women, children and adolescents, including: