Responding to COVID-19 while protecting essential services for women, children and adolescents
Vacant beds, vacant chairs, and dusty floors. Unused IV stands, along with other medical equipment sitting in the corner. Empty hospital wards that were once crowded with mothers and children seeking care.
Since the onset of the COVID-19 pandemic, this had been a common sight in many health facilities across Kinshasa, the capital of Democratic Republic of Congo (DRC). Between March and July 2020, the number of patients visiting health facilities dropped dramatically from 70% to 25%. Fears of contracting COVID-19 prevented parents from taking their children to hospitals and clinics while many pregnant women chose to postpone ante-natal care services and routine immunizations. Lockdowns made it more difficult for women to move around, either because of lack of childcare or transportation.
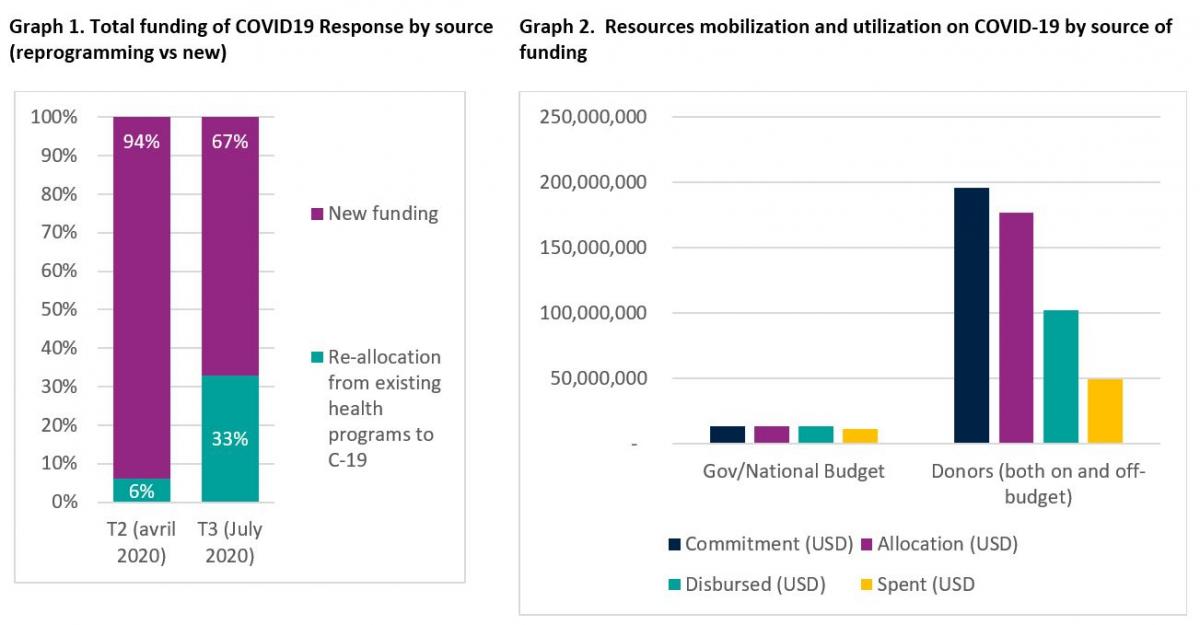
Demand for services was not the only impact on the health system. Funding for routine, lifesaving health services for women, children and adolescents also dropped sharply as resources were shifted to the country’s COVID-19 emergency response efforts. This shift seems to be increasing over time – in April 2020, only 6% of the health budget was reprogrammed to the COVID-19 response; by October, it had grown more than five-fold to 33% (Graph 1).
Understanding the resource landscape
An effective response to COVID-19 has meant mobilizing additional resources and re-programming existing resources, while ensuring efficient and fast flow of funds. However, diverting funding from lifesaving services can result in service disruptions, leaving millions of women and children at risk of dying or enduring lifelong impacts.
In the early days of the pandemic, the DRC’s Ministry of Health initiated a COVID-19 Response Plan resource mapping and expenditure tracking exercise (RMET), with support from the Global Financing Facility (GFF), the World Health Organization (WHO), the World Bank and other partners. The process rapidly collects data on health and COVID-19-related budget commitments, disbursements, and expenditures from several sources to help governments monitor resource availability and spending on routine health services and track investment in health systems.
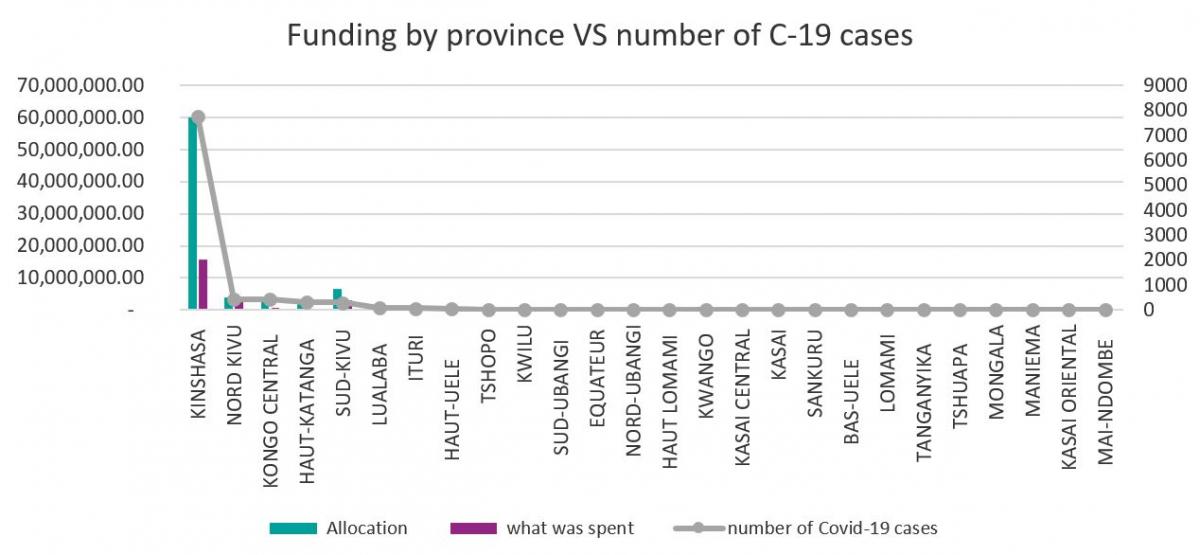
Data from this exercise provided valuable information to DRC’s Ministry of Health. It helped monitor whether partner and domestic funding for COVID-19 could be secured without jeopardizing implementation of the national health strategy, which already faced a 50% funding gap before the outbreak. The RMET exercise also enabled the ministry to assess funding needs and understand which of the plan’s pillars were under-funded or over-funded. It also shed light on resource allocations to geographic areas with the greatest need. For example, it showed that the five provinces most affected by COVID-19 received the most funding, with Kinshasa receiving the highest allocation since it struggled with the highest number of cases (Graph 3). Finally, RMET helped the government understand how efficiently the budget was executed, prompting the ministry to take action to address bottlenecks (Graph 2).
A tool for all
DRC is not alone in trying to respond to the COVID-19 crisis while managing other priorities across its entire health system, such as the continuation of lifesaving services for women, children and adolescents. Other countries, like Ghana, have also taken steps to assess their current resource needs. In an environment of increasing pressures to deliver health care for all and to show greater transparency and accountability when using additional funding, more and more countries are seeking reliable data to make smart decisions.
To respond to the knowledge gap and increasing country demand for technical support, the GFF, WHO, the World Bank, Gavi, and the Global Fund jointly produced a technical brief - RMET for COVID-19 Response: A Design Checklist and Overview of Tools. The brief, which aims to inform policymakers and development partners designing and implementing RMET for COVID-19 responses, sheds light on the following:
- How to define country needs for COVID-19 RMET: including examples of how resource mapping data can be used to strengthen COVID-19 responses
- Designing a “fit for purpose” RMET exercise – a checklist and design tradeoff considerations for countries that seek to improve an existing RMET exercise or for countries that are assessing technical requirements for an upcoming exercise for COVID-19 response
- Overview of available tools – for countries embarking on RMET for COVID-19, or would like to change their current methodologies and are assessing available tools and resources
The WHO and GFF have jointly designed a RMET data collection tool for COVID-19 and for broader national health strategies, which is currently being piloted in Niger. At the global level, WHO and OECD are jointly collaborating on a methodology for mapping COVID-19 expenditures with the SHA2011 classifications.
While these tools and resources are a first step towards stronger decision-making, country stakeholders need to systematize this process and promote stronger data governance, accountability and transparency.