
Tanzania
CASE STUDY
Tanzania
Tanzania recorded major improvements in several RMNCAH-N outcomes in the decade between 2005 and 2015 (Box 1). At the same time, progress on some indicators has been mixed, with significant regional variations. Tanzania’s commitment to improving maternal, newborn, child, and adolescent health and nutrition (RMNCAH-N) outcomes is evidenced by the country’s commitment to join the GFF.
In a bid to improve RMNCAH-N outcomes, the country has continued to strengthen its work with partners to coordinate the financing and implementation of RMNCAH-N programs aimed at improving the quality and coverage of health services in alignment with its investment case, One Plan II.1 This collaborative effort has led to improvements in maternal and child health service coverage, quality, and services, as measured by the indicators that have been routinely monitored and are described in this case study. The findings also highlight that to continue progress toward further RMNCAH-N improvements, more targeted efforts are needed to expand the coverage of some services (ANC4+, for example) in certain regions where coverage remains below 50 percent while sustaining the quality improvements that have been recorded in the last two years.

Trends in key RMNCAH-N indicators (2005 to 2015, DHS)
- Maternal mortality ratio:
Declined from 578 to 556 per 100,000 live births - Neonatal mortality rate:
Declined from 32 to 25 deaths per 1,000 live births - Under-five mortality rate:
Declined from 112 to 67 deaths per 1,000 live births - Stunting prevalence among children under five:
Declined from 44.3 to 34.4 percent - Wasting prevalence among children under five:
Rose from 3.0 to 4.4 percent - Share of women who had another child less than 24 months after their previous child:
Rose from 16 to 18 percent - Total fertility rate:
Declined from 5.7 to 5.2 children per woman
Country Priorities: One Plan II
One Plan II, Tanzania’s investment case, focuses on improving RMNCAH-N with an emphasis on improving the quality and availability of health services to reduce morbidity and mortality. One Plan II is implemented on the premise of the Government of Tanzania’s vision of increasing local ownership by giving health facilities greater autonomy to make decisions about service provision and quality of care and relieving health system bottlenecks through mechanisms that provide direct financing to facilities linked to results. This model is meant to empower frontline providers and health facility managers to improve quality and access to healthcare services, while basing their financing on the achievement of results and context-specific health priorities. In addition, it increases accountability at the community level by giving the oversight and stewardship functions to each facility’s governing committee. Further, the reliance and focus on data use enables facilities to plan, monitor, and develop solutions relevant to their specific regions.
The GFF’s engagement in Tanzania has evolved into support for health systems strengthening activities and data use that can contribute to improvements in coverage, quality, and access to services. Specifically, these include (i) alignment of partners around a common domestic health financing agenda and better coordination to reduce fragmentation in allocation of funds; (ii) co-financing of One Plan II through the results-based Primary Health Care for Results (PHCforR) program; and (iii) support for a mid-term review of One Plan II.
Alignment of partners around a common domestic resource mobilization agenda and coordination for better allocation of funds
The Government of Tanzania spends 7 percent of its general budget on healthcare, according to a public expenditure review. Government spending still represents just 28 percent of total health spending in the country, with the remainder provided by donors (37 percent), households (26 percent), and a prepayment scheme (9 percent). Although government expenditure for health as a percentage of general government budget is modest, retaining or increasing the level of domestic government expenditure is a critical goal in Tanzania. High-level consultative meetings with the Ministry of Health and Parliamentarians were held to discuss the importance of increasing domestic resources from the government, which has enhanced the Ministry of Health’s ability to advocate for more funding for the sector. The GFF and the World Bank have been supporting this health financing objective through a specific disbursement-linked indicator (DLI) aiming to increase domestic funding for health over time.
To reduce fragmentation of funding, a government-led RMNCAH technical working group and a Sector-Wide Approach technical working group, which focuses on the financial side, together form the country platform in Tanzania. Enhancing efficiency, pooling of resources, and strategic purchasing, especially at the facility level, are priorities for both the partners and the Government of Tanzania. Harmonized planning and spending guidelines for facilities, to be applied to all sources of funds at the facility level, further strengthen this effort.
Financial support to One Plan II through the results-based Primary Health Care for Results (PHCforR) program
The GFF Trust Fund is co-financing One Plan II through the PHCforR program, which ties funding to improved health outcomes at all levels of service delivery using DLIs. USAID, the Power of Nutrition, and the World Bank and GFF Trust Fund all provide financing through the PHCforR up to the facility level through innovative approaches, such as output-based payment modalities, to improve RMNCAH-N outcomes.
The DLI indicators are used in scorecards to measure the performance of local government authorities, which helps inform their joint annual planning, which is also supported by the Health Basket Fund. Twelve criteria are featured in the scorecard, corresponding to key challenges or bottlenecks that affect the quality of care in Tanzania, as identified by the government. These 12 criteria include six criteria covering maternal, neonatal, and child health and nutrition service delivery outputs, and another six that cover quality of care. The local government authority scorecards support local-level accountability while also promoting a systematic and continuous monitoring of achievements and gaps for RMNCAH coverage indicators aligned with One Plan II.
To improve facilities’ performance in terms of quality of service delivery, the Star Rating initiative has been used. The Star Rating system is a nationwide ranking of health facilities whose scoring ranges from 0 to 5 stars and includes criteria that correspond to improvements in the conditions for the provision of quality care and that facilitate the achievement of maternal, neonatal and child health service delivery outcomes. The Star Rating Initiative includes a quality improvement plan as well as efforts to help health facilities achieve improved structural quality of care. Criteria included in the rating include human resources for health, availability of essential drugs, social accountability, and completeness of data entry.
Midterm review of One Plan II
Tanzania will be the first GFF country to complete a midterm review of its investment case. The objective of this review is to track progress, learn from successes as well as failures, and identify strategies to realign activities so that One Plan II better achieves the objectives laid out in its results framework. Specific focus areas of the review include understanding the bottlenecks that hinder progress, identifying highly vulnerable populations that are not being reached, and mapping out a clear path for the way forward. In parallel, support is provided for Tanzania to conduct a new resource mapping and tracking activity to identify financial gaps in One Plan II financing. Results from the resource mapping and the midterm review will be critical to informing the realignment of the plan.
Results
The results in One Plan II are partially financed through DLIs in the PHCforR program; as such, expected results in both documents are in direct alignment. Results in both the investment case and the PHCforR focus on all levels of the health system, with the end goal of improving the quality and availability of RMNCAH-N services to reduce morbidity and mortality.
To date, Tanzania has experienced significant improvements in many of the coverage, quality, and service improvement indicators that are central to the One Plan II and the PHCforR results frameworks. These results have been routinely monitored through the local government authority scorecards and Star Ratings Initiative, and demonstrate improvements in many indicators, among them: coverage of antenatal care, facility-based births, presence of a skilled staff member, and quality of services delivered during antenatal care visits. Quality of care is ultimately represented in the types of services received at the health facility, but improvements in star ratings under the Star Rating Initiative further attest to this progress.
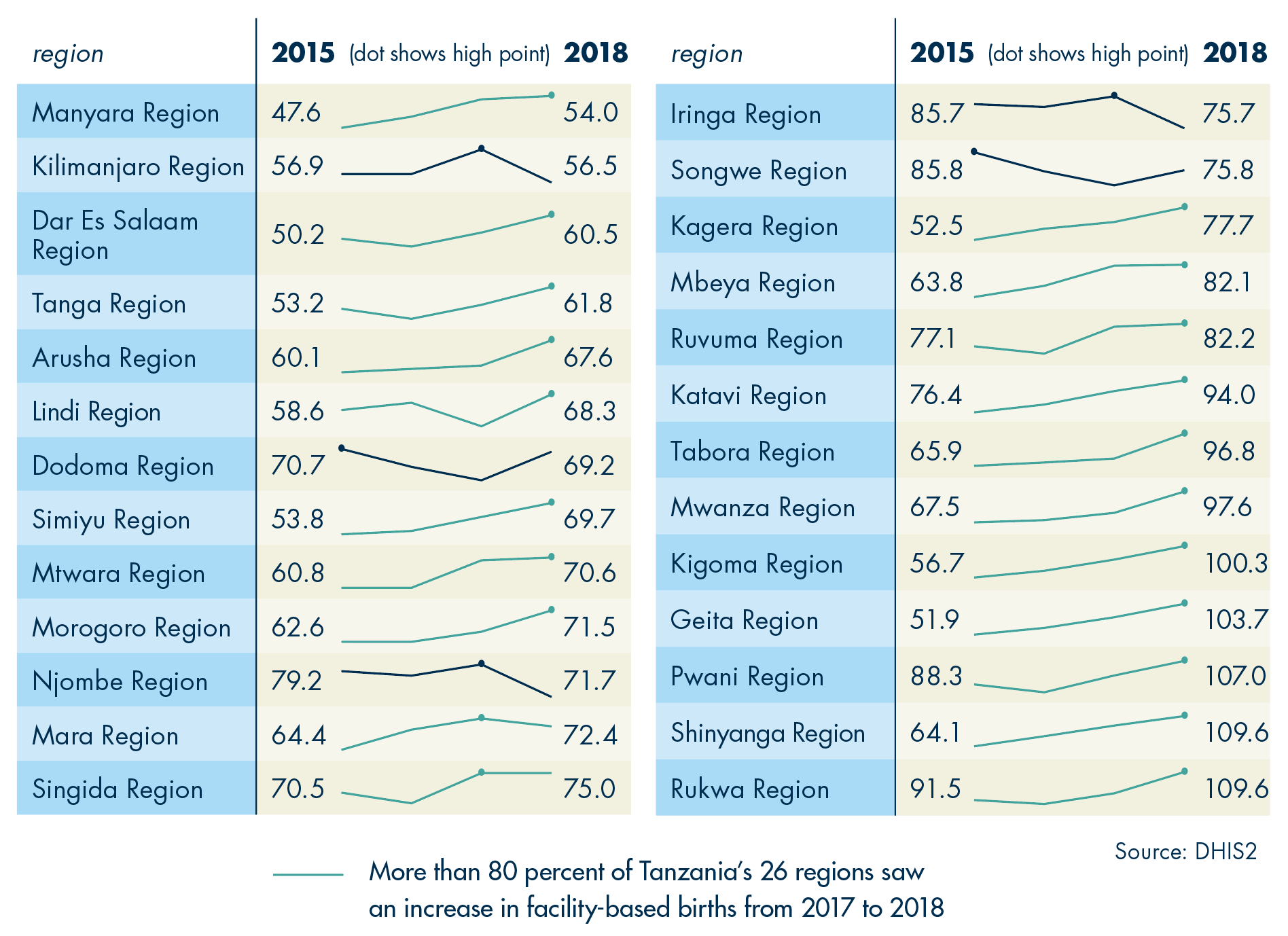
Antenatal care improved in all 26 regions, from an average of 35.8 percent of pregnant women receiving at least four antenatal care visits in 2014 to 64.1 percent in 2018 (Figure 1). Increases are in response to some regions seeing more than 70 percent attendance in ANC (Dar Es Salaam, Geita, Katavi, Kigoma, Mbeya, Pwani, Rukwa, and Shinyanga). Nevertheless, many regions remain below 50 percent coverage of ANC4+, highlighting the need for efforts on both the demand and supply side to increase coverage. Alongside improvements in ANC4+ coverage were increases in the regional averages for the share of births at a health facility, which rose from 67.0 percent in 2014 to 70.6 percent in 2017, and to 79.6 percent in 2018 (Figure 2) (RMNCAH Bulletin 2019).
Figure 1
Percent of women in Tanzania receiving at least four antenatal visits, by region, 2014–18
In almost one-third of Tanzania’s regions, at least 70% of pregnant women are reached with ANC4+, but in many other regions coverage is under 50%

Figure 2
Percent of facility-based births in Tanzania, by region, 2014–18
Parallel increases in coverage of intermittent preventive treatment (IPT) of malaria and in the administering of iron and folic acid signal improvements not only in the coverage of ANC services but also in the quality of those services. The proportion of pregnant women who received IPT2 between 2014 and 2018 climbed from 36.4 percent to 82.8 percent. IPT3 was introduced in 2016; its use reached 59 percent by 2018 (data not presented). As shown in Figure 3, the average share of pregnant women receiving iron and folic acid at ANC visits increased from 57 percent in 2014 to 75 percent in 2018, with a large majority of regions achieving coverage of iron and folic acid distribution during ANC above 70 percent.
Figure 3
Percent of pregnant women in Tanzania receiving iron and folic acid, by region, 2014–18
More than 70% of pregnant women in a majority of regions in Tanzania received iron and folic acid in 2018

Further attesting to quality improvements is the increase in the number of facilities that achieved at least a 3-star rating between 2016 and 2018 (Figure 4). In 2016, 137 facilities achieved a 3-star rating or higher; this number climbed to 1,370 facilities by 2018. This is equivalent to an increase in the average proportion of facilities achieving at least a 3-star rating from 0.9 percent in 2016 to 18 percent in 2018. In 2018, the highest-performing region saw 41.1 percent of its facilities achieving a 3-star rating, while the lowest-performing region saw just 2.8 percent of its facilities perform at this level.
Figure 4
Percent of facilities in Tanzania that received at least a 3-star rating, by region, 2014–18

The increases in the number of facilities with three-star ratings reflect how both RMNCAH-N coverage and quality of care have increased in Tanzania over the past two years. However, district and regional results still reflect variations in performance, which highlight the need to learn from regions that are making the greatest progress and apply those lessons, where relevant, to poorer performing regions.